Fear & Loathing in the Temporal Lobes
Correlates of So-Called Spiritual Experiences with Sub-Clinical Epilepsy
by Iona Miller, ©2003

"Tricksters", Iona Miller, 24x36, 1993
Our minds can trick us by importing cultural narratives to explain our anomalous experiences in terms of our spiritual beliefs. Such self-reports often overlook physiological or neurological conditions that foster such ideas
based on our subjective experience.
based on our subjective experience.
Abstract: The origins of individuality can be found in neurological correlates and even in pathologies. Abnormalities in the temporal lobes (TLE) caused by genetics, injury, or infections can lead to amplification of spiritual characteristics in the personality. Temporal lobe seizures mimic or perhaps even embody certain essentially religious experiences. While neurology cannot explain away spiritual consciousness it can describe some of its mechanisms, adding to self-understanding. The limbic system helps control our homeostatic “set points” for temperature, sleep, body fat and behavioral urges like sex drive and aggression.
This tendency may be reinforced by a kindling process potentiating pathways to the amygdala and other parts of the brain. Part of the limbic system, the amygdala performs a primary role in the processing of anxiety, memory modulation, consolidation and emotional arousal, learning and reactions. Strength of memory and attributed meaning are consolidated. It also relates to sexual orientation, fear, and aggression. The inferior temporal lobe, including the amygdala and hippocampus are also involved in the formation of dream images, hallucinations, and feelings of familiarity.
Emotional tone and multisensory content of these experiences is dependent on which lobe (right or left) and portion of the temporal lobes become unstable and subject to seizures, clincal or sub-clinical. Electrical stimulation of the right amygdala induces negative emotions, especially fear and sadness, while stimulation of the left amygdala induces either rewarding pleasure (happiness) or unpleasant (fear, anxiety, sadness) emotions. Danger signaling stimuli overcome the amygdala's typical set point. Changes in hedonic set point can lead to cravings or compulsive drug-seeking and drug-taking behavior characteristic of addiction.
Thus, we experiences 'angels' or 'demons'. Left temporal lobe hallucination may involve single words, verbal monologues, sentences, commands, advice, or distant conversations which can't quite be made out. Such experiences affect our worldview and sense of self and others. Set point thresholds for stress reactions in sensitive individuals or those with early trauma are lower. Studies show meditation helps modulate the amygdala. Frequently the same melody is heard over and over, or the sound of singing voices and individual instruments.
Similarly, complex visual and emotional hallucinations, such as typified by dream imagery or psychedelics, is associated with the right temporal lobe. The interconnected amygdala, hippocampus, and temporal lobe appear to act in concert during mystical experience. Hyperactivation infuses perceptions with tremendous religious and emotional feeling, endowing it with special or religious significance.
The phenomena which appear pathologically in TLE can also appear in the general population, and are often even encouraged by the practice of meditation. Sel-soothing calms the amygdala, reducing effects of trauma. The union of brain science and theology is called neurotheology which studies all related religious and spiritual phenomena and their neurological roots. Persinger, Murphy (2013) and others have reproduced many anomalous experiences, including near-death experiences, alien presence, and other perceptual apparitions in the laboratory by applying electromagnetic frequencies to particular parts of the brain.
This tendency may be reinforced by a kindling process potentiating pathways to the amygdala and other parts of the brain. Part of the limbic system, the amygdala performs a primary role in the processing of anxiety, memory modulation, consolidation and emotional arousal, learning and reactions. Strength of memory and attributed meaning are consolidated. It also relates to sexual orientation, fear, and aggression. The inferior temporal lobe, including the amygdala and hippocampus are also involved in the formation of dream images, hallucinations, and feelings of familiarity.
Emotional tone and multisensory content of these experiences is dependent on which lobe (right or left) and portion of the temporal lobes become unstable and subject to seizures, clincal or sub-clinical. Electrical stimulation of the right amygdala induces negative emotions, especially fear and sadness, while stimulation of the left amygdala induces either rewarding pleasure (happiness) or unpleasant (fear, anxiety, sadness) emotions. Danger signaling stimuli overcome the amygdala's typical set point. Changes in hedonic set point can lead to cravings or compulsive drug-seeking and drug-taking behavior characteristic of addiction.
Thus, we experiences 'angels' or 'demons'. Left temporal lobe hallucination may involve single words, verbal monologues, sentences, commands, advice, or distant conversations which can't quite be made out. Such experiences affect our worldview and sense of self and others. Set point thresholds for stress reactions in sensitive individuals or those with early trauma are lower. Studies show meditation helps modulate the amygdala. Frequently the same melody is heard over and over, or the sound of singing voices and individual instruments.
Similarly, complex visual and emotional hallucinations, such as typified by dream imagery or psychedelics, is associated with the right temporal lobe. The interconnected amygdala, hippocampus, and temporal lobe appear to act in concert during mystical experience. Hyperactivation infuses perceptions with tremendous religious and emotional feeling, endowing it with special or religious significance.
The phenomena which appear pathologically in TLE can also appear in the general population, and are often even encouraged by the practice of meditation. Sel-soothing calms the amygdala, reducing effects of trauma. The union of brain science and theology is called neurotheology which studies all related religious and spiritual phenomena and their neurological roots. Persinger, Murphy (2013) and others have reproduced many anomalous experiences, including near-death experiences, alien presence, and other perceptual apparitions in the laboratory by applying electromagnetic frequencies to particular parts of the brain.
Introduction
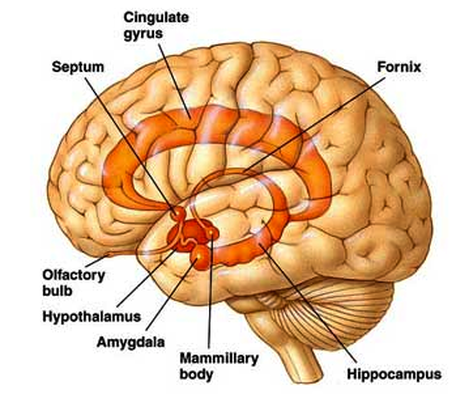
The origins of individuality can be found in neurological correlates. We all have a cortex, hypothalamus, hippocampus (gateway to memory and integration of outer and inner reality), amygdala (mediates motivation, affect and and meaning), and limbic system (emotional center).
However, there are variations in their dynamics from individual to individual for a variety of psychophysical reasons. A tangle of genetic, neuroendocrinal, and neurochemical roots, as well as psychological or physical traumatic experiences, underlie many behavioral anomalies.
The brain regulates the functioning of the body through the release of hormones, and those hormones, in turn, regulate the functioning of the brain. Thus, clusters of neurons carry on complex operations, which influence organs and glands throughout the body, as information moves from one end of a neuron to another and across plastic synaptic junctions.
Populations of neurons interact through excitatory and inhibitory neurotransmitters. Individual distinctions can be seen in stress responses by inhibition and long-term potentiation of neural networks.
Behavioral biology plays an important role in individual behavior. Our biology challenges us on many levels from survival and adaptation to cherished beliefs and deepest fears. We cannot predict our inner world any more than we can predict the world around us.
Complex cultural settings determine how much of a problem manifestations of these anomalies are for each person. Disorders that were once called witchcraft, demonic possession or thought divine now have medical or neuropsychiatric names with biological explanations.
The biological continuum describes all individuals but provides no clear definition of what is “normal.” Often it is difficult to determine where “normal” stops and “abnormal” begins. This is particularly the case when sub-clinical, non-epileptic (NES) or mini-seizures affect the temporal lobe of the brain.
Among the most electrically unstable portions of the brain, the temporal lobes are quite sensitive to extremely low magnetic frequencies (Persinger). There is a continuum of temporal lobe lability or sensitivity, and even normal individuals have sub-clinical microseizures frequently, particularly during REM or dreams. The full-blown effects of such electrical storms are seen in petit mal and grand mal seizures of epilepsy.
Epileptic seizures propagate across the brain through a process called “kindling.” Nerve signals are amplified exponentially, resulting in a chaotic electrical storm that can entrain more than one brain area. For example, in temporal lobe epilepsy, spreading includes the temporal lobe, underlying limbic structures and hippocampus; all of them fire in an overexcited manner, especially if serotonin levels are low.
Epilepsy is triggered by different parts of the brain. Behavioral changes immediately preceding an epileptic seizure indicate what portion of the brain is the focus of the seizure. Electrical lability, or seizures in the temporal lobes do not usually cause physical convulsions, unless they propagate to the motor regions.
The temporal lobes host many structures and functions including memory, orientation of self in space and time, interpretations of meaning and emotional significance, organization of audio and visual patterns, smell, and language. Local discharges can be potentiated by specific memory recall or extremely low biofrequency magnetic fields penetrating brain tissue.
Temporal lobe epilepsy (TLE) is accompanied by classic personality changes. Though some researchers disagree, attributed characteristics include the following: loss of humor; intense affect; moodswings (peaks or highs, depressions, distortions, aggression); suggestibility; existential anxiety; neophobia; hypergraphia; an intense active interest in dreams, religion and philosophy; reports of psi experiences. Supreme faith is placed in the validity of subjective experience. They accept logical incongruities, displaying a rigid core of private beliefs.
This later spiritual interest can be rooted in subjective experiences of a variety of phenomena kindled by electrical instabilities in the brain. They include, but are not limited to depersonalization, time distortion, anxiety or panic, floating or falling sensations, peripheral imagery, a sense of presence either sacred or malefic, apparitions, downloading of memory sequences and false memory confabulations or fantasies, voices and visionary experiences ranging from heavenly to hellish, and a panoply of psychophysical manifestations.
With TLE, unusual experiences are assigned special personal meaning. We all like to believe we are unique individuals unlike anyone who has ever existed. Our self-images are conditioned by our multisensory interpretations of our experiences and feedback from others as well as our existential situation. The limbic system, which determines how actively we engage our environment, is conditioned by early developmental history as well as other factors.
The amygdala, or “emotional sentinel”, is “calibrated” through early subjective perceptions of what it is like to be in the world, whether it is safe and cozy, or toxic and threatening (Goleman). Such conditioning could begin in the womb where the fetus is subject to both the emotional and biochemical reactions and indulgences of the mother. If the womb is toxic the fetus perceives this in a multisensory way that may condition self-image.
Fear Factor
We all have fears, but some of us experience periods of time when we feel overwhelmed by either vague or specific fears and anxieties. The autonomic system is regulated by emotions as well as thoughts, not to mention the fight/flight responses of sympathetic arousal.
Among all the upsetting notions humans can experience, perhaps the fear of death is at the top of the list. Our mortality is a difficult prospect to contemplate; yet the evidence clearly surrounds us. Death always stands at the ready or rides piggyback with us, ready to be our advisor, whispering in our ear, making its presence known. Even denial cannot keep the natural foreboding at bay.
Confrontations with death aroused superstitious and spiritual feelings in our ancient ancestors that led from increasingly elaborate burial procedures, to shamanic practices to assuage unknown powers, and eventually to the growth of the world’s major religions with their notions of finer planes of existence and the varieties of afterlife.
Coupled with powerful experiential episodes, such as mystic transport with and without shamanic plants, near-death experiences and grave illness, strong beliefs arose within the heart of humanity. They were shared with others becoming fixed ideas, philosophies and organized religions. Historically, perhaps more wars have been fought over competing ideologies than over territory.
Fear of death or powerful subjective experiences can also lead to idiosyncratic spiritual ideas and practices. Again neural networks come into play as the bases of memory, pain, coping, and creativity.
The focus sharpens when one loses self-esteem and self-identity through loss of confidence and “control” in the performance of the body or perceptions of the mind. Both come powerfully into play in epilepsy. This can create a strong sense of conviction, destiny, fate or even mission, which will be aggressively defended.
Is it possible to identify epilepsy as a true cause of sudden religious conversion, such as Saul of Tarsus becoming Paul on the road to Damascus, or the deep convictions of Muhammad who wrote the Koran after the onset of his seizures, or the voices and divine visions of Moses, Ezekiel, St. Teresa of Avila, Swedenborg, Kierkegaard, even Joseph Smith? Black Elk had seizures before his grand “buffalo” vision.
Could a simple head injury, infection or mutation in a single gene, for example, lead to such a fundamental shift or revelation in worldview? TLE is a mixed blessing at best, perhaps at the core of many noted artists and religious figures. TLE shapes the personality, the self-concept. Vast depolarizng waves cascade across the brain. As well as intense periods of creativity and euphoria there may be periods of panic or fear for no reason, even confusion, hallucinations, and rage.
The temporal lobe plays a key role in emotional stability. It interprets and integrates input to give it meaning, in the deeply emotional rather than intellectual sense. Of course not every unusual experience, religious impulse, or bright idea comes from faulty electrical action and cascading seizures, or they would would lose all meaning.
Rapture of the Neurological Deep
How do we get from existential anxieties about death to intensely personal spiritual experience? Many of our spiritual notions come from the reports of the dying, or those with near-death experiences (NDEs). When the brain begins to shut down certain typical experiences appear as each of the major areas of the brain crash and billions of functional neurons heave their last gasp (McKinney).
Deeply embedded neurons in the brainstem are among the last to go. Unless the brain is physically destroyed, dying is a process. It doesn’t instantly collapse, but degrades in a somewhat predictable manner with associated characteristic phenomena.
Meanwhile, there is a regression toward the oceanic feelings of life in the womb as the process of birth gets played in reverse and we return to eternity. We journey back through earlier forms of consciousness, in a dreamy haze once the frontal lobes cease their rationalizing and abstractions.
As in dreams there are irregular bursts of neural static and discharge (Hobson) that affect the visual, affective, motor, orientation, time, and memory areas. There is no more chronological sequencing of events. Our experience of dying is synthesized holistically from the confabulation of all these elements. We may be unconscious and yet still somewhat aware with scintillating electrical surges creating their last faltering messages as they fail.
We dissociate from the body. As in deep meditation, attention is withdrawn from the extremities and external senses. We return to a simpler mode of being, the undifferentiated mind, where time seems endless, if it exists at all. As oxygen levels drop, and opiate-like endorphins are dumped into the system, the sense of peace and contentment may rise along with our spirits. Phantasmogorical images flood our awareness.
Between the dissociation from the body and the last glimpse of light, we may experience a culturally conditioned transcendence. Some might say the soul leaves the body as it journeys into the Light. Bright white light may be the melding of all colors of the visual spectrum once the visual cortex is disinhibited.
Perhaps as many as 1/3 of those coming close to death report a characteristic cluster of experiences. Bruce Greyson, in a paper in Varieties of Anomalous Experience (Cardena et al), lists the common elements of adult near-death experiences and aftereffects:
Ineffability
Hearing oneself pronounced dead
Feelings of peace and quiet
Hearing unusual noises
Seeing a dark tunnel
Being “out of the body”
Meeting “spiritual beings”
Experiencing a bright light as a “being of light”
Panoramic life review
Experiencing a realm in which all knowledge exists
Experiencing cities of light
Experiencing a realm of bewildered spirits
Experiencing a “supernatural rescue”
Sensing a border or limit
Coming back “into the body”
Frustration relating experiences to others
Subtle “broadening and deepening” of life
Elimination of fear of death
Corroboration of events witnessed while “out of the body”
The reports of those with near-death experiences moving through a tunnel toward the light, accompanied by ancestors, deceased friends and their cultural divinities are now well known (Ring; Moody; Sabom). A minority experience emotional problems requiring psychosocial rehabilitation following NDEs, including anger and depression at having been “returned” perhaps unwillingly, broken relationships, disrupted career, alienation, post-traumatic stress disorder, “social death” (Greyson).
Gradual death is often gentle, creating its own palliative. Heavens and hells are fully immersive virtual reality constructions of our dying neural networks. But when the brain comes close to an irreversible coma on the journey towards death, the great endarkening comes before any great enlightenment. Hence many with NDEs do not report seeing the Light and may even focus on their experiences as being intensely negative in content and tone.
Unable to calm their disoriented mind, their dismal experience is largely one of panic, pain, and terror. This may be the result of toxins in the blood including carbon dioxide buildup. If we die a sudden violent death, we may miss heaven, but mercifully we will never know that.
The whole process may be greatly compounded by the release of powerful endogenous hallucinogenic DMT from the pineal gland (Strassman). In highly stressful situations, such as birth, sexual ecstasy, extreme physical distress, childbirth, near-death and death, the normal inhibitions against the production and circulation of this potent mind-bending “spirit molecule” are over-ridden. Massive DMT dumps may also create intense visions of blinding white light, ecstatic emotions, timelessness, and powerful presence.
A neurobiological model proposed by Saavedra-Aguilar and Gomez-Jeria suggests temporal-lobe dysfunction, hypoxia, psychophysical stress, and neurotransmitter changes combine to induce epileptiform discharges in the hippocampus and amygdala. They contribute to life review and and complex visual hallucinations.
When the visual cortex begins to crash (Blackmore), there is a cascade of distorted imagery, then a shift down the color spectrum toward primeval redness and impenetrable black. Maybe there is still a dull glow or scintillating pinpoints of light, like stars in some inner universe.
As the reticular activating system dies there may be a final burst of distant light, somehow familiar from the very dawn of our existence. As our last cells die, the mind is finally unwound. We have closed the circle of life and entered the Great Beyond.
TLTs and the Spiritual Personality
Are some people predisposed to psychism, mystical visions, or religious zeal? What lies at the root of the personality driven to pursue the spiritual quest, often characterized as a “seeker”? How does one come by an intensely personal, even idiosyncratic relationship with either gods or demons, aliens or nature spirits? Are we hardwired for religious beliefs?
The shamanic personality, which is characterized by an early mental and physical healing crisis, is typically considered to have “a foot in both worlds,” the ordinary and the Great Unknown. It is this quality that makes them able to “journey” to other worlds, the underworld, or the heights. Euphoria and ecstasies come coupled with anxiety and incapacitating terror.
The psychic quality opens them to dreamlike voices and visions, premonitions, ancestral and spectral images and communications, as well as an ability to pass into and return from the realm of the dead. Feelings of oneness with all life can nurture personalities that are charismatic and create instant and powerful rapport, even spontaneous trance states and healing in others. Shamans, nature mystics or medicine people were leaders within their tribal societies.
All these qualities are correlated with the sub-clinical and TLE syndrome. Can this possibly have given rise to the ancient notion that the “falling sickness” was a “divine” disorder, dictated by the gods? Some great leaders, such as Julius Caesar, were perceived as immortals; despite the infirmity; it did not diminish and may have increased their personal power. Rather than bipolar, was Joan of Arc experiencing non-epileptic seizures or left-lobe epilepsy?
Does their seeming fearlessness arise from the intimate knowledge of the eternal “otherside.” Memory works by tapping neural networks necessary to find the information. Temporal episodes, overlapping projections of networks, can simultaneously “download” unrelated memories creating seemingly new meaningful feeling-colored experiences. They correlate with “fugue states”, flashbacks, beatific states, oceanic consciousness, and cosmic insights.
Ramachandran attributes increased emotional intensity to the kindling or potentiating of the pathway between the temporal lobe and amygdala, heightening the significance of stimuli. What is deemed meaningful becomes extraordinarily meaningful. Images of religious images or words can even be preferred over those of a sexual nature.
Some parts of the brain can block input into others. When certain portions of the brain are inhibited, such as the cingulate gyrus and orientation center, out of body experiences create a sense of floating or transport. When the parietal lobe is blocked of sensory input sense of self and world merges. The hippocampus no longer provides a “reality check.” Loss of sense of time leads to atemporal reveries and ecstasies. When cascades spread across the brain, they can entrain the auditory, visual, olfactory, or taste centers.
Overdriving the frontal cortex with induced pain, concentration or steady, regular stimulation to the CNS enhances the effect leading to disinhibition. Personal crisis, oxygen deprivation, low blood sugar, repressed serotonin levels, or fatigue amplify the process. In neurological terms, sensitization is a term meaning a stimulus that did not have an effect on the ANS now does. The effects, either anomalous or from meditation, can be spontaneous or cumulative.
This, of course, also relates directly to stress-induced syndromes. Neuroelectrical activity cranked up beyond a certain threshold creates travelling and rotating waves that form complex interference patterns (Mandell). Physical and psychological stress can cause changes in the amount of hormones secreted, affecting general health and reproductive interest and ability. Conversely hormones affect the brain.
TICKLING THE GOD MODULE
We are wired to experience God. Different researchers have slightly different names for the religious syndrome. Ramachandran calls it “the God module.” Persinger calls it the “God experience”. Both researchers indicate waves of temporal lobe excitation with hemispheric coherence underlie spiritual experience and religious belief. “The Kingdom of heaven is within.”
It is reported Dostoevsky said his seizures gave him “feelings of magnificence, abundance, eternity.” Poe and Lewis Carrol brought their novel distorted perceptions into their writing to the delight of millions. Van Gogh was prolific, though tormented, unconnective, and codependent. Writers from Tennyson to Philip K. Dick have turned their infirmity to their advantage.
When they could easily moderate them with anticonvulsants, many individuals still choose to endure their symptoms rather than relinquish glimpses of the psychic fireworks it brings. Still, neuroscientists are the first to admit that God is not reduceable to a neuroelectrical flux. But stress, particularly loss of a loved one, definitely facilitates the God experience. Elevated stress hormones can trigger the temporal lobe, amygdala, and hippocampus.
Persinger has tickled the temporal lobes of enough individuals to define the parameters of electromagnetic shifts on brain function. The recent medical use of Transcranial Magnetic Stimulation (TMS) to relieve a variety of psychological symptoms such as depression indicates that the mind may be an electromagnetic field.
Not all those with intense spiritual experiences have temporal lobe epilepsy. Meditators often sit for years before experiencing the slightest tingles or visions of light. But often once manifestations begin, they increase in frequency and tend to stabilize. They can come as sounds, smells, intense feeling, visonary landscapes or forms of living entities, or amorphous lights. These inner experiences feel as real or seem more real than external perception.
The study of how the brain creates god experiences is the province of the embryonic field of neurotheology. As the marriage of brain science with theology, it systematically describes the relationship between humans, God and the universe in neurological terms (Miller, 2003).
But just because we can say the brain declares, “Let there be God,” doesn’t mean a higher power does not exist. When God said, “Let there be Light,” perhaps it also meant the electrical impulses that vivify, provide meaning and enlighten our mundane existence. Visions cannot be judged solely on the neurological basis but must be judged for their own merit and validity. Not all visions are pathological, nor all visionaries or spiritual adepts epileptics.
Subjective experiences are the basis of mysticism and the religious impulse. The brain is hard-wired for mystical experiences, perhaps as an adaptation to soothe the stress incured in daily life. Peak experiences, raptures, epiphanies, even illumination are potentially available to everyone. Spontaneous transient electrical choas in the temporal lobes is perfectly normal, making the God experience an artifact of healthy function.
We can learn to make space, time and personality dissolve. Fear dissolves too as we kiss the feet of eternity. All we have to do is withdraw our attention from the senses and interrupt certain brain circuits. These experiences can also be induced neuromagnetically with new technologies, and non-invasively with “brainwave drivers” such as the frequency-following response or binaural beat technology (Monroe).
The god experience is a process in which one learns to embody spiritual being, infusing life with meaning. The soul soars, freed from the prison of ego, mind and body. It brings in its wake oceanic expansion, suspension of time, space and ego, sudden insight, childlike wonder, exaltation, gnosis, fusion.
Appendix & References Appendix A: The TLE Syndrome
TLE is often undiagnosed as subjects often forget a simple but crucial injury to the head, even in childhood, such as falling down stairs, car wrecks, swimming injuries, or a host of other everyday bumps and jolts. The soft temporal lobes are vulnerable to injury any time they bump against the hard skull.
Dr. Daniel Amen says temporal lobe functions include auditory processes, ventral visual stream, auditory input, visual object recognition and classification, long term storage of sensory input. It links with the amygdala which adds the emotional tone to sensory input and memories. The hippocampus helps us navigate and determine where we are in space.
Primary functions of the dominant side (usually the left) include perception of words and processing of language related sounds, sequential analysis, increased blood flow during speech perception, processing details, intermediate and long term memory, auditory learning and retrieval of words, visual and auditory processing, and complex memories.
So instabilities or damage to the left lobe create problems such as emotional instability, decreased verbal memory, difficulty categorizing words or pictures, failing to understand words in context, internally and externally driven aggression, dark or violent thoughts, sensitivity to slights and mild paranoia, auditory processing problems, and reading difficulties.
Non-dominant side (usually the right) temporal functions include perception of melodies, pitch and rhythm, social cues, reading facial expressions, and vocal intonation, visual learning, and increased blood flow during tonal memory. Problems include recall of shapes, faces, and tunes; inept social skills, trouble reading social cues and context; decreased attention to visual input; trouble processing music and visual imagery.
Problems in either or both lobes create troubles with memories, fears, confusion, anxiety, abnormal sensory perceptions, visual and auditory hallucinations, spaciness or amnesia, déjà vu and jamais vu, unusual abdominal pain or headaches, religious or moral preoccupation, excessive writing, overemphasis on trivia, and of course seizures.
Dr. Amen sums up the symptomology with ten defining points: 1). Disturbance of auditory sensation and perception; 2). Disturbance of selective attention of auditory and visual input; 3). Disorders of visual perception; 4). Impaired organization and categorization of verbal material; 5). Disturbance of language comprehension; 6). Decreased long term memory; 7). Altered personality and affective development; 8). Altered sexual behavior; 9). Inability to perceive or remember events; 10). Damage to the inferior aspect of the temporal lobe – decreased memory in proportion to tissue damaged.
APPENDIX B
Personal Philosophy Inventory (Makarec and Persinger, 1990)
(Sample items indicating complex partial epileptic temporal lobe signs.)
While sitting quietly, I have had uplifting sensations as if I were driving over a rolling road.
I often feel as if things are not real.
At least once, before falling down, I had an intense smell from childhood, apparently for no reason.
Once, in a crowded place, I suddenly could not recognize where I was.
I have had a vision.
People tell me I "blank out" sometimes when we're talking.
When relaxed or before falling asleep I sometimes feel pleasant vibrations moving through my body.
Sometimes in the very early morning hours I have meaningful experiences.
I have heard an inner voice call my name.
I use hunches more than simple learning to solve new problems.
Sometimes an event occurs that has special significance for me only.
I have had experiences where I felt as if I were somewhere else.
There have been brief times when I felt very close to a Universal Consciousness.
I have had dreams of floating or flying through the air.
At least once in my life I have felt the presence of another being.
(Sample items indicating Psi experiences or exotic beliefs)
I have been taken aboard a space ship.
I would like to time travel.
When I have a tough decision a sign will be given and I will know what to do.
If God told me to kill, I would do it in His name.
I think there is a good possibility that I have lived a previous life.
Telepathy is a real phenomenon.
An inner voice has told me where to find something and it was there.
Alien intelligence is probably responsible for UFOs.
I have felt as if I have left my body.
*****
APPENDIX C
Subjective Experiences Questionnaire (Ruttan, Persinger and Koren, 1990) {exit survey}
( Sample items indicating targeted experiences test for vestibular, depersonalization, and imaginings.)
I felt dizzy or odd.
I felt the presence of someone or something near me.
There were tingling sensations.
I saw vivid images.
There were pleasant vibrations moving through my body.
I heard an inner voice call my name or speak to me.
I experienced anger.
I experienced sadness.
The experience did not come from my own mind.
I heard a ticking sound.
There were odd smells.
I experienced terror or fear.
There were odd tastes in my mouth.
I felt as if I were somewhere else.
I experienced thoughts from childhood.
The same idea kept occurring.
I felt as if I were spinning around.
There were images from dreams I've had.
The red light became brighter or darker.
REFERENCES
Amen, Daniel C. (19 ). Change Your Brain, Change Your Life.
Amen, Daniel C. (19 ). Healing Anxiety and Depression.
Amen, Daniel C.(19 ). Healing the Hardware of the Soul:How Making the Brain-Soul Connection Can Optimize Your Life, Love and Spiritual Growth.
Bear, D. M. and Fedio, P. (1977). Quantitative Analysis of Interictal Behavior in Temporal Lobe Epilsepsy,” Archives of Neurology, 34, 1977, pp.454-467.
Begley, Sharon (2001). “Religion and the Brain”. Newsweek, April, 2001.
Blackmore, Susan (1993). Dying to Live: Near-Death Experiences. Buffalo, NY: Prometheus.
Cardena, Etzel, Lynn, Steven Jay, and Krippner, Stanley (eds.) (2001). The Varieties of Anomalous Experience. Washington D.C.: American Psychological Assn.
Cirignotta, F., Todesco, C. V., & Lugaresi, E. (1980). Temporal lobe epilepsy with ecstatic seizures (so-called Dostoevskian Epilepsy). Epilepsia, 21, 705-710.
Csikszentmihalyi, Mihaly (1990). Flow: The Psychology of Optimal Experience. New York: Harper & Row.
Gloor, P. (1982-1986). “Role of the Human Limbic System in Perception, Memory, and Affect: Lessons from Temporal Lobe Epilepsy,” Annals of Neurology, 12, 1982, pp, 129-144. Also in The Limbic System, Doane and Livingston (eds.). New York: Raven (1986).
Goleman, Daniel (1995). Emotional Intelligence. New York: Bantam.
Hobson, Alan (1998). Consciousness. Scientific American Press.Hooper, Judith and Tersi, Dick (1986). The Three-Pound Universe. New York: Tarcher/G. P. Putnam’s Sons.
Horgan, John (2003). Rational Mysticism. New York: Houghton Mifflin Company.
Huot, B., Makarec, K. & Persinger, M.A. (1989). Temporal Lobe Signs and Jungian Dimensions of Personality. Perceptual and Motor Skills, 69, 841-842.
LaPlante, Eve (1994). Seized.
Makarec, K., & Persinger, M. A. (1985). Temporal lobe signs: Electroencephalographic validity and enhanced scores in special populations. Perceptual and Motor Skills, 60, 831-842.
Makarec, K., & Persinger, M. A. (1990). Electroencephalographic validation of a temporal lobe signs inventory in a normal population. Journal of Research in Personality, 24, 323-337.
Mandell, Arnold (1980). “Toward a Psychobiology of Transcendence: God in the Brain” on Davidson & Davidson (eds.), The Psychobiology of Consciousness. New York: Plenum Press.
Marshall, E. J., Syed, G. M. S., Fenwick, P. B. C., & Lishman, W. A. (1993). A pilot study of schizophrenia-like psychosis in epilepsy using single photon emission computerized tomography. British Journal of Psychiatry, 163, 32-36.
Maturana, U. & Varela, F. (1987). The Tree of Knowledge: the Biological Roots of Human Understanding. Shambala: Boston.
McKinney, Laurence O.(1994). Neurotheology: Virtual Religion in the 21st Century. Cambridge, Mass.: American Institute for Mindfulness.
Munro, C., & Persinger, M. A. (1992). Relative right temporal lobe theta activity correlates with Vignanos Hemispheric Quotient and the sensed presence. Perceptual and Motor Skills, 75, 899-903.
Murphy, Todd (2013), Sacred Pathways: The Brain's Role in Religious and Mystical Experiences.
Niedermeyer, E. (1982). Epileptic seizure disorders. In Niedermeyer & F. L. da Silva (Eds.) Electroencephalography: Basic Principles, Clinical Applications and Related Fields, Baltimore-Munich: Urban & Swartzenberg. Pp. 339-428.
Miller, Iona (2001). “Neurotheology 101: Our Innate Capacity for Spiritual or Mystical Experience”. Asklepia Foundation.
Miller, Iona (2003). “How the Brain Creates God: the Emerging Science of Neurotheology,” Chaosophy 2003. Grants Pass, Oregon: Asklepia Press.
Moody, R.A. (1975). Life After Life. Covington, Ga.: Mockingbird Books.
Monroe, Robert
Okamura, A. O., Fukai, M., Yamadori, A., Hidari, M., Asaba, H., & Sakai, T. (1993). A clinical study of hypergraphia in epilepsy. Journal of Neurology, Neurosurgery, and Psychiatry, 56, 556-559.
Perez, M. M., Trimble, M. R., Murray, N. M. F., & Reider, I. (1985). Epileptic psychosis: An evaluation of PSE profiles. British Journal of Psychiatry, 146, 155-163
Persinger, M. A. (1975). “ELF Waves and ESP”; New Horizons, I(5), January 1975, pp.232-235.
Persinger, M. A. , (1983). Religious and mystical experiences as artifacts of temporal lobe function. Perceptual and Motor Skills, 57, 1255-1262.
Persinger, M. A. , (1984). Striking EEG profiles from single episodes of glossolalia and transcendental meditation. Perceptual and Motor Skills, 58, 963-975.
Persinger, M. A. , (1984). People who report religious experiences may also display enhanced temporal lobe signs. Perceptual and Motor Skills. 58, 963-975.
Persinger, M. A. , (1985). Geophysical variables and human behavior: XXX. Intense paranormal experiences occur during days of quiet, global geomagnetic activity. Perceptual and Motor Skills, 61, 320-322.
Persinger, M. A., & Valliant, P. M. (1985). Temporal lobe signs and reports of subjective paranormal experiences in a normal population: A replication. Perceptual and Motor Skills, 60, 903-909.
Persinger, Michael A. (1987). Neuropsychological Bases of God Beliefs. New York: Praeger Publishers.
Persinger, M. A. and Makarec, K. (1987). “Temporal Lobe Epilsepsy Signs and Correlative Behaviors Displayed by Normal Populations,” Journal of General Psychology, 114, 1987, pp. 179-185.
Persinger, M. A. , (1988). Temporal lobe signs and personality characteristics. Perceptual and Motor Skills, 66, 49-50.
Persinger, Michael (1989). “Psi Phenomena and Temporal Lobe Activity: The Geomagnetic Factor,” in L.A. Henkel and R. E. Berger (eds.), Research in Parapsychology 1988; Metuchen, NJ: Scarecrow Press, 1989.
Persinger, M. A., & Fisher, S. D. (1990). Elevated, specific temporal lobe signs in a population engaged in psychic studies. Perceptual and Motor Skills, 71, 817-818.
Persinger, M. A., Koren, S. A., Makarec, K., Richards, P., & Youlton, S. (1991). Differential effects of wave form and the subjects possible temporal lobe signs upon experiences during cerebral exposure to weak intensity magnetic fields. Journal of Bioelectricity, 10(1&2), 141-184.
Persinger, M. A. , (1991). Subjective pseudocyesis (false pregnancy) and elevated temporal lobe signs: An implication. Perceptual and Motor Skills, 72, 499-503.
Persinger, M. A. , (1993). Transcendental meditation and general meditation are associated with enhanced complex partial epileptic-like signs: Evidence for cognitive kindling? Perceptual and Motor Skills, 76, 80-82.
Pribram, Karl H. (1971). Languages of the Brain: Experimental Paradoxes and Principles in Neuropsychology. Monterey, Calif.: Brooks/Cole Publishing Co.
Ramachandran, Vilayanur (1998). Phantoms in the Brain.
Richards, P. M., Koren, S. A., & Persinger, M. A. (1992). Experimental stimulation by burst-firing weak magnetic fields over the right temporal lobe may facilitate apprehension in women. Perceptual and Motor Skills, 75, 667-670.
Ring, Kenneth (1984). “The Nature of Personal Identity in the Near-Death Experience”. Anabiosis 4(1) (Spring 1984).
Ruttan, L. A., Persinger, M. A. & Koren, S. A. (1990). Enhancement of temporal lobe-related experiences during brief exposures to milligauss intensity extremely low frequency magnetic fields. Journal of Bioelectricity, 9(1), 33-54.
Ryvlin, P., Philipon, B., Cinotti, L., Froment, J. C., LeBars, D., & Mauguiere, F. (1992). Functional neuroimaging strategy in temporal lobe epilepsy: A comparative study of 18FDG-PET and 99MtC-HMPAO- SPECT. Annals of Neurology, 31(6), 650-656.
Saavedra-Aguilar, J.C. & Gomez-Jeria, J.S. (1989). “A Neurobiological Model for Near-Death Experiences.” Journal of Near-Death Studies, 7, 205-222.
Sabom, M (1982). Recollections of Death: A Medical Investigation. New York: Harper & Row.
Sabom, M. (1998). Light and Death: One Doctor’s Fascinating Account of Near-Death Experiences. Grand Rapids, MI: Zondervan.
Salzman, Mark. Lying Awake.
Strassman, Rick (1997). “Endogenous ketmine-like compounds and the NDE…” Journal of Near-Death Studies, 16, 27-41.
Strassman, Rick (2001). DMT: The Spirit Molecule. Rochester, Vermont: Park St. Press.
Varela, F., Thompson, E. & Rosch, E. (1991). The Embodied Mind. MIT Press: Boston.
Waller, N. G., Kojetin, B. A., Bouchard Jr., T. J., Lykken, D. T., & Tellegen, A. (1990). Genetic and environmental influences on religious interests, attitudes and values. Psychological Science, 1(2), 138-142.
File Created: 9-14-03
Extended References:
Allen, J., & Lester, D. (1994). Belief in paranormal phenomena and an external locus of control. Perceptual and Motor Skills, 79, 226.
Arango, M. A. , & Persinger , M. A. (1988). Geophysical variables and behavior: LII. Decreased geomagnetic activity and spontaneous telepathic experiences from the Sidgwick collection. Perceptual and Motor Skills, 67, 907-910.
Ardilla, A. (1989). Partial cognitive seizures . Neuropsychiatry, Neuropsychology, and Behavioral Neurology, 2(3), 175-182.
Berger, R. E., & Persinger , M. A. (1991). Geophysical variables and behavior: LXVII. Quieter annual geomagnetic activity and larger effect size for experimental psi (ESP) studies over six decades. Perceptual and Motor Skills, 73, 1219-1223.
Brewerton, T. D. (1994). Hypereligiosity in psychotic disorders. The Journal of Nervous and Mental Disease, 182(5), 302-304.
Gillis, C., & Persinger, M. A. (1993). Shifts in the Plutchik Emotion Profile indices following three weekly treatments with pulsed Vs continuous cerebral magnetic fields. Perceptual and Motor Skills, 76, 168-170.
Hopping, M. (1984). Psychic seizures: A diagnostic challenge. Bulletin of the Menninger Clinic, 48(5), 401-417.
Kalat, J. W. (1995). Biological Psychology (5th. Ed.). Pacific Grove: Brookes/Cole.
Kumar, V. K., Pekala, R. J., & Cummings, J. (1993). Sensation seeking, drug use and paranormal beliefs and experiences. Personality and Individual Differences, 14(5), 685-691.
Ogunyemi, A. O., & Breen, H. (1993). Seizures induced by music. Behavioral Neurology, 6, 215-218.
Pederson, D. M. (1994). Identification of levels of self-identity. Perceptual and Motor Skills, 78, 1155-1167.
Persinger, M. A. , (1983). Geophysical variables and human behavior: VII. Specific prediction of UFO reports within the New Madrid states by solar-geomagnetic and seismic measures. Perceptual and Motor Skills, 56, 243-249.
Persinger, M. A. , (1992). Neuropsychological profiles of adults who report sudden remembering of early childhood experiences: Implications for claims of sex abuse and alien visitation/abduction experiences. Perceptual and Motor Skills, 75, 254-266.
Persinger, M. A. , (1993). Average diurnal changes in melatonin levels are associated with hourly incidence of bereavement apparitions: Support for the hypothesis of temporal (limbic) lobe microseizuring. Perceptual and Motor Skills, 76, 444-446.
Persinger, M. A. , (1993). Geophysical variables and human behavior: LXXI. Differential contribution of geomagnetic activity to paranormal experiences concerning death and crises: An alternative to the ESP hypothesis. Perceptual and Motor Skills, 76, 555-562.
Persinger, M. A., & Derr, J. S. (1984). Geophysical variables and human behavior: XIX. Strong temporal relationships between inclusive seismic measures and UFO reports within Washington state. Perceptual and Motor Skills, 59, 551-566.
Persinger, M. A., & Levesque, B. F. (1983). Geophysical variables and human behavior: XII. The weather matrix accommodates large portions of variance of measured daily mood. Perceptual and Motor Skills, 57, 868-870.
Rank, O. (1971). The Double: A Psychoanalytic Study, trans. by Harry Tucker Jr., Chapel Hill: University of North Carolina.
Richards, P. M., Persinger, M. A. & Koren, S. A. (1993). Modification of activation and evaluation properties of narratives by weak complex magnetic field patterns that simulate limbic burst firing. International Journal of Neuroscience, 71, 71-85.
Schaut, G. B., & Persinger, M. A. (1985). Geophysical variables and human behavior: XXXI. Global geomagnetic activity during spontaneous paranormal experiences: A replication. Perceptual and Motor Skills, 61, 412-414.
Tobacyk, J. J., & Wilkinson, L. V. (1991). Paranormal beliefs and preferences for games of chance. Psychological Reports, 68, 1088-1090.
Waller, N. G., Kojetin, B. A., Bouchard Jr., T. J., Lykken, D. T., & Tellegen, A. (1990). Genetic and environmental influences on religious interests, attitudes and values. Psychological Science, 1(2), 138-142.
The current hypothesis is that Positron Emission Tomography can demonstrate which specific limbic structures are involved in the expression of these altered states on an approximately linear relationship between the continuum of emotionality and the continuum of involvement of cerebral structures ranging from cortical temporal lobe to hippocampal/amygdaloid structures to core basal limbic structures; in effect, the deeper the activation, the deeper the emotion. Retention of the null hypothesis would require either a) subjects who represent a normal population demonstrate no affective experiences on the SEQ as a result of the stimulus, or b) affective experiences are reported but limbic regions are not shown to be involved.
NEAR DEATH EXPERIENCE RESEARCH
http://www.stnews.org/News-787.htm
Having a near death experience can change a person’s entire life, including one’s brain, researchers have discovered.
Researcher Willoughby Britton, a doctoral student at the University of Arizona, studied the brain waves of people who have had positive, transformative near death experiences and found their brain patterns distinctive when compared with people who didn’t have a brush with death.
“It’s interesting to see why some people are transformed and why some people aren’t and whether studying people with positive near death experiences can help the people who have negative experiences,” Britton said. “It’s a profound personality overhaul.”
Britton compared the brainwaves of sleeping subjects and found a distinct spike in activity in the temporal lobe of people with near death experiences.
The brain’s temporal lobe has often been implicated in reports of near death experiences that closely mirror what epileptics feel during a seizure: feelings of peace and tranquility, encountering a bright light and increased sensitivity to smells and sounds.
The temporal lobe, Britton said, is considered “the God module, the part of the brain that connects with the transcendent.” Surprisingly, however, all of the activity that Britton recorded was from the left half of the brain not the right half, which is more often associated with visual and spatial creativity.
“One hundred percent of the activity came from the left side, which, in itself, is very unusual,” said Britton. “There’s no reason for someone to have an accident and just have one side of their brain affected.”
All those in Britton’s study who came close to dying scored higher on an evaluation of their ability to cope with stressful situations than their counterparts.
http://query.nytimes.com/gst/fullpage.html?sec=health&res=9D06E4DE1E38F930A25757C0A9629C8B63
The scientists assumed that the near-death group would show patterns of brain activity similar to those seen in temporal lobe epileptics, who often describe undergoing spiritual out-of-body events during seizures. The abnormal activity, however, did not spring up in the right temporal lobe, as is sometimes the case with epilepsy. Instead, the activity appeared almost exclusively in the left temporal lobe.
Unexpectedly, the researchers also found that the participants, like many people who suffer depression, had abnormal sleep patterns. But unlike people with depression, who move unusually quickly into the rapid eye movement or REM phase of sleep, the subjects who reported near-death experiences took an unusually long time to move into REM.
PDF: Near-Death Experiences and the Temporal Lobes by Willoughby Britton
http://matrix.aklab.psych.ubc.ca/uploads/Amelia_Neardeath_PS.pdf#search=%22temporal%20lobes%20willoughby%20britton%22
Perceptual and Motor Skills, 1983, 57, 1255-1262. © Perceptual and Motor Skills 1983
RELIGIOUS AND MYSTICAL EXPERIENCES AS ARTIFACTS OF
TEMPORAL LOBE FUNCTION: A GENERAL HYPOTHESIS
Micheal A. Persinger
Laurentian University
Summary: Mystical and religious experiences are hypothesized to be evoked by transient, electrical microseizures within deep structures of the temporal lobe. Although experiential details are affected by context and reinforcement history, basic themes reflect the inclusion of different amygdaloid-hippocampal structures and adjacent cortices. Whereas the unusual electrical coherence allows access to infantile memories of parents, a source of god expectations, specific stimulation evokes out-of-body experiences, space-time distortions, intense meaningfulness, and dreamy scenes. The species-specific similarities in temporal lobe properties enhance the homogeneity of cross- cultural experiences. They exist along a continuum that ranges from “early morning highs” to recurrent bouts of conversion and dominating religiosity. Predisposing factors include any biochemical or genetic factors that produce temporal lobe lability. A variety of precipitating stimuli provoke these experiences, but personal (life) crises and death bed conditions are optimal. These temporal lobe microseizures can be learned as responses to existential trauma because stimulation is of powerful intrinsic reward regions and reduction of death anxiety occurs. The implications of these transients as potent modifiers of human behavior are considered.
The neuropsychological basis of religious experiences and God beliefs has avoided by behavioral scientists. Yet these experiences, in conjunction the confrontation and attenuation of death anxiety, constitute a major class of human behaviors whose frequency is rivaled only by sex and aggression. This paper briefly describes a general hypothesis that religious and mystical experiences are normal consequences of spontaneous biogenic stimulation of temporal lobe structures. The numbers, composition, and intensity of these experiences reflect a continuum of temporal lobe stability. Each human being may be located somewhere along this dimension.
The temporal lobe of the human brain is an optimal locus for the creation of religious experiences. Cortical and deep structures (primarily the amygdaloid and hippocampal complexes) are associated with the sense of “self” in relationship to time and space, the memory-dependent conception of their limits primary affective components of anticipation, especially of nociceptive events. Given copious inputs from languaging centers (Gloor, 1972), all of these experiences are influenced by suggestion and by the rich imagery-evoking sequences of metaphorical language. It is not surprising that anticipation of self-dissolution, death anxiety, would emerge within this context.
Deep telencephalic structures have acquired particular importance in human development. Experiences of self and the propensity for self-preservation have been elaborated upon the general amygdaloid role of hypothalamic modulation. The amygdala contains representations of motivational states and their affective (pleasure or reward versus pain or punishment) dimensions. Whereas crude (and wide spread) stimulation evokes fear (Weingarten, Cherlow, & Holmgren, 1977) and general anxiety (anticipation of negative stimuli), more subtle stimulation evokes intense meaningfulness and peak experiences; the latter are often in conjunction with altered body perceptions, such as out-of-body experiences (Jasper & Rasmussen, 1958) or convictions of cosmic communion.
Intricate and highly organized connections between deep structures and the overlying associative cortices allow complex memories and language to control the evocation of amygdaloid experiences. Consequently, they can be infused with the details of context and determined by the expectancy of the person. Plentiful opiate receptor sites in this portion of the amygdala and along the temporal pole (Pay, 1982) allow positive experiences to be influenced by a chemical dimension that ranges from synthetic substances (morphine derivatives) to the enkephalin physiology of life crises.
Considering the direct connections to the dorsomedial portions of the thalamus and orbital frontal lobes, time distortions (e.g., viewing eternity in a split second) would not be unexpected. Sudden amygdaloid stimulation and alteration of the sense of self in space-time could momentarily alter hippocampal function and change memory reference. The alteration may range from institution of memories that appear to be “old and real” to the conviction that something meaningful and intensely personal has happened (although the details are vague). A significant portion of them would be characterized by a long latency between the time of the experience and its report.
Three important physiological properties target the temporal lobe as the source of mystical/religious experiences. Post-stimulation electrical instability, an intrinsic feature of deep structures, allows the creation of transient neuronal firing patterns that do not necessarily represent concurrent sensory input. Instead, they could incorporate combinations of memory and fantasy, but still within the context of the moment. This region is well known for its capacity to generate learned seizures (kindling); antithetically, conditioned inhibition of seizure patterns, is also predictable and has been observed (Efron, 1957).
Second, these areas are prone to vascular anomalies such as transient vasospasms. They are now considered a primary cause of hallucinatory experiences (Altura & Altura, 1981). The recent evolutionary changes in the position of Ammon’s horn, including the formation of an extra gyrus to accommodate this development, has fostered vasospasmogenic potential due to the odd cytoarchitecture. This is enhanced by the conspicuous coronal asymmetry of the Sylvian fissures (LeMay, 1982) which contribute to unusual electrical discrepancies between the two hemispheres.
The plasticity of temporal lobe neuronal and glial populations are exceptional. Cellular membranes in this region are prone to both interneuronal and neuronal-glial fusion, an important predisposing factor to psychomotor epilepsy (Schwartzkroin, 1983); within less extreme conditions, it aids unusual mixtures of cell ensembles. They can be affected by vitamin B deficiencies, hormonal fluctuations, hypoglycemia, hypoxia, and tumorogenesis, to which these structures are particularly sensitive (Breggin, 1979). Although postnatal neurogenesis has not been clearly demonstrated in man, this area displays environmental-dependent alterations in dendritic arborbization that are evident even by light microscopy (Buell & Coleman, 1979).
According to the hypothesis, the actual mystical or religious experience is evoked by a transient (a few seconds), very focal, electrical display within the temporal lobe. Such temporal lobe transients (TLTs) would be analogous to electrical microseizures without any obvious motor components; some facial expressions, such as ecstasy and occasional lacrimation would be noticeable. Lip smacking, facial distortions, automatisms, and vagal glossopharyngeal-mediated vocalization (speaking in tongues), followed by amnesia, would occur in more extreme conditions. Although most TLTs should be subcortical in origin, some would be represented within electroencephalic (EEG) profiles. They would be characterized by local, perhaps even lead- specific, transient, seizure-like signatures surrounded by normal activity.
The origins of individuality can be found in neurological correlates. We all have a cortex, hypothalamus, hippocampus (gateway to memory and integration of outer and inner reality), amygdala (mediates motivation, affect and and meaning), and limbic system (emotional center).
However, there are variations in their dynamics from individual to individual for a variety of psychophysical reasons. A tangle of genetic, neuroendocrinal, and neurochemical roots, as well as psychological or physical traumatic experiences, underlie many behavioral anomalies.
The brain regulates the functioning of the body through the release of hormones, and those hormones, in turn, regulate the functioning of the brain. Thus, clusters of neurons carry on complex operations, which influence organs and glands throughout the body, as information moves from one end of a neuron to another and across plastic synaptic junctions.
Populations of neurons interact through excitatory and inhibitory neurotransmitters. Individual distinctions can be seen in stress responses by inhibition and long-term potentiation of neural networks.
Behavioral biology plays an important role in individual behavior. Our biology challenges us on many levels from survival and adaptation to cherished beliefs and deepest fears. We cannot predict our inner world any more than we can predict the world around us.
Complex cultural settings determine how much of a problem manifestations of these anomalies are for each person. Disorders that were once called witchcraft, demonic possession or thought divine now have medical or neuropsychiatric names with biological explanations.
The biological continuum describes all individuals but provides no clear definition of what is “normal.” Often it is difficult to determine where “normal” stops and “abnormal” begins. This is particularly the case when sub-clinical, non-epileptic (NES) or mini-seizures affect the temporal lobe of the brain.
Among the most electrically unstable portions of the brain, the temporal lobes are quite sensitive to extremely low magnetic frequencies (Persinger). There is a continuum of temporal lobe lability or sensitivity, and even normal individuals have sub-clinical microseizures frequently, particularly during REM or dreams. The full-blown effects of such electrical storms are seen in petit mal and grand mal seizures of epilepsy.
Epileptic seizures propagate across the brain through a process called “kindling.” Nerve signals are amplified exponentially, resulting in a chaotic electrical storm that can entrain more than one brain area. For example, in temporal lobe epilepsy, spreading includes the temporal lobe, underlying limbic structures and hippocampus; all of them fire in an overexcited manner, especially if serotonin levels are low.
Epilepsy is triggered by different parts of the brain. Behavioral changes immediately preceding an epileptic seizure indicate what portion of the brain is the focus of the seizure. Electrical lability, or seizures in the temporal lobes do not usually cause physical convulsions, unless they propagate to the motor regions.
The temporal lobes host many structures and functions including memory, orientation of self in space and time, interpretations of meaning and emotional significance, organization of audio and visual patterns, smell, and language. Local discharges can be potentiated by specific memory recall or extremely low biofrequency magnetic fields penetrating brain tissue.
Temporal lobe epilepsy (TLE) is accompanied by classic personality changes. Though some researchers disagree, attributed characteristics include the following: loss of humor; intense affect; moodswings (peaks or highs, depressions, distortions, aggression); suggestibility; existential anxiety; neophobia; hypergraphia; an intense active interest in dreams, religion and philosophy; reports of psi experiences. Supreme faith is placed in the validity of subjective experience. They accept logical incongruities, displaying a rigid core of private beliefs.
This later spiritual interest can be rooted in subjective experiences of a variety of phenomena kindled by electrical instabilities in the brain. They include, but are not limited to depersonalization, time distortion, anxiety or panic, floating or falling sensations, peripheral imagery, a sense of presence either sacred or malefic, apparitions, downloading of memory sequences and false memory confabulations or fantasies, voices and visionary experiences ranging from heavenly to hellish, and a panoply of psychophysical manifestations.
With TLE, unusual experiences are assigned special personal meaning. We all like to believe we are unique individuals unlike anyone who has ever existed. Our self-images are conditioned by our multisensory interpretations of our experiences and feedback from others as well as our existential situation. The limbic system, which determines how actively we engage our environment, is conditioned by early developmental history as well as other factors.
The amygdala, or “emotional sentinel”, is “calibrated” through early subjective perceptions of what it is like to be in the world, whether it is safe and cozy, or toxic and threatening (Goleman). Such conditioning could begin in the womb where the fetus is subject to both the emotional and biochemical reactions and indulgences of the mother. If the womb is toxic the fetus perceives this in a multisensory way that may condition self-image.
Fear Factor
We all have fears, but some of us experience periods of time when we feel overwhelmed by either vague or specific fears and anxieties. The autonomic system is regulated by emotions as well as thoughts, not to mention the fight/flight responses of sympathetic arousal.
Among all the upsetting notions humans can experience, perhaps the fear of death is at the top of the list. Our mortality is a difficult prospect to contemplate; yet the evidence clearly surrounds us. Death always stands at the ready or rides piggyback with us, ready to be our advisor, whispering in our ear, making its presence known. Even denial cannot keep the natural foreboding at bay.
Confrontations with death aroused superstitious and spiritual feelings in our ancient ancestors that led from increasingly elaborate burial procedures, to shamanic practices to assuage unknown powers, and eventually to the growth of the world’s major religions with their notions of finer planes of existence and the varieties of afterlife.
Coupled with powerful experiential episodes, such as mystic transport with and without shamanic plants, near-death experiences and grave illness, strong beliefs arose within the heart of humanity. They were shared with others becoming fixed ideas, philosophies and organized religions. Historically, perhaps more wars have been fought over competing ideologies than over territory.
Fear of death or powerful subjective experiences can also lead to idiosyncratic spiritual ideas and practices. Again neural networks come into play as the bases of memory, pain, coping, and creativity.
The focus sharpens when one loses self-esteem and self-identity through loss of confidence and “control” in the performance of the body or perceptions of the mind. Both come powerfully into play in epilepsy. This can create a strong sense of conviction, destiny, fate or even mission, which will be aggressively defended.
Is it possible to identify epilepsy as a true cause of sudden religious conversion, such as Saul of Tarsus becoming Paul on the road to Damascus, or the deep convictions of Muhammad who wrote the Koran after the onset of his seizures, or the voices and divine visions of Moses, Ezekiel, St. Teresa of Avila, Swedenborg, Kierkegaard, even Joseph Smith? Black Elk had seizures before his grand “buffalo” vision.
Could a simple head injury, infection or mutation in a single gene, for example, lead to such a fundamental shift or revelation in worldview? TLE is a mixed blessing at best, perhaps at the core of many noted artists and religious figures. TLE shapes the personality, the self-concept. Vast depolarizng waves cascade across the brain. As well as intense periods of creativity and euphoria there may be periods of panic or fear for no reason, even confusion, hallucinations, and rage.
The temporal lobe plays a key role in emotional stability. It interprets and integrates input to give it meaning, in the deeply emotional rather than intellectual sense. Of course not every unusual experience, religious impulse, or bright idea comes from faulty electrical action and cascading seizures, or they would would lose all meaning.
Rapture of the Neurological Deep
How do we get from existential anxieties about death to intensely personal spiritual experience? Many of our spiritual notions come from the reports of the dying, or those with near-death experiences (NDEs). When the brain begins to shut down certain typical experiences appear as each of the major areas of the brain crash and billions of functional neurons heave their last gasp (McKinney).
Deeply embedded neurons in the brainstem are among the last to go. Unless the brain is physically destroyed, dying is a process. It doesn’t instantly collapse, but degrades in a somewhat predictable manner with associated characteristic phenomena.
Meanwhile, there is a regression toward the oceanic feelings of life in the womb as the process of birth gets played in reverse and we return to eternity. We journey back through earlier forms of consciousness, in a dreamy haze once the frontal lobes cease their rationalizing and abstractions.
As in dreams there are irregular bursts of neural static and discharge (Hobson) that affect the visual, affective, motor, orientation, time, and memory areas. There is no more chronological sequencing of events. Our experience of dying is synthesized holistically from the confabulation of all these elements. We may be unconscious and yet still somewhat aware with scintillating electrical surges creating their last faltering messages as they fail.
We dissociate from the body. As in deep meditation, attention is withdrawn from the extremities and external senses. We return to a simpler mode of being, the undifferentiated mind, where time seems endless, if it exists at all. As oxygen levels drop, and opiate-like endorphins are dumped into the system, the sense of peace and contentment may rise along with our spirits. Phantasmogorical images flood our awareness.
Between the dissociation from the body and the last glimpse of light, we may experience a culturally conditioned transcendence. Some might say the soul leaves the body as it journeys into the Light. Bright white light may be the melding of all colors of the visual spectrum once the visual cortex is disinhibited.
Perhaps as many as 1/3 of those coming close to death report a characteristic cluster of experiences. Bruce Greyson, in a paper in Varieties of Anomalous Experience (Cardena et al), lists the common elements of adult near-death experiences and aftereffects:
Ineffability
Hearing oneself pronounced dead
Feelings of peace and quiet
Hearing unusual noises
Seeing a dark tunnel
Being “out of the body”
Meeting “spiritual beings”
Experiencing a bright light as a “being of light”
Panoramic life review
Experiencing a realm in which all knowledge exists
Experiencing cities of light
Experiencing a realm of bewildered spirits
Experiencing a “supernatural rescue”
Sensing a border or limit
Coming back “into the body”
Frustration relating experiences to others
Subtle “broadening and deepening” of life
Elimination of fear of death
Corroboration of events witnessed while “out of the body”
The reports of those with near-death experiences moving through a tunnel toward the light, accompanied by ancestors, deceased friends and their cultural divinities are now well known (Ring; Moody; Sabom). A minority experience emotional problems requiring psychosocial rehabilitation following NDEs, including anger and depression at having been “returned” perhaps unwillingly, broken relationships, disrupted career, alienation, post-traumatic stress disorder, “social death” (Greyson).
Gradual death is often gentle, creating its own palliative. Heavens and hells are fully immersive virtual reality constructions of our dying neural networks. But when the brain comes close to an irreversible coma on the journey towards death, the great endarkening comes before any great enlightenment. Hence many with NDEs do not report seeing the Light and may even focus on their experiences as being intensely negative in content and tone.
Unable to calm their disoriented mind, their dismal experience is largely one of panic, pain, and terror. This may be the result of toxins in the blood including carbon dioxide buildup. If we die a sudden violent death, we may miss heaven, but mercifully we will never know that.
The whole process may be greatly compounded by the release of powerful endogenous hallucinogenic DMT from the pineal gland (Strassman). In highly stressful situations, such as birth, sexual ecstasy, extreme physical distress, childbirth, near-death and death, the normal inhibitions against the production and circulation of this potent mind-bending “spirit molecule” are over-ridden. Massive DMT dumps may also create intense visions of blinding white light, ecstatic emotions, timelessness, and powerful presence.
A neurobiological model proposed by Saavedra-Aguilar and Gomez-Jeria suggests temporal-lobe dysfunction, hypoxia, psychophysical stress, and neurotransmitter changes combine to induce epileptiform discharges in the hippocampus and amygdala. They contribute to life review and and complex visual hallucinations.
When the visual cortex begins to crash (Blackmore), there is a cascade of distorted imagery, then a shift down the color spectrum toward primeval redness and impenetrable black. Maybe there is still a dull glow or scintillating pinpoints of light, like stars in some inner universe.
As the reticular activating system dies there may be a final burst of distant light, somehow familiar from the very dawn of our existence. As our last cells die, the mind is finally unwound. We have closed the circle of life and entered the Great Beyond.
TLTs and the Spiritual Personality
Are some people predisposed to psychism, mystical visions, or religious zeal? What lies at the root of the personality driven to pursue the spiritual quest, often characterized as a “seeker”? How does one come by an intensely personal, even idiosyncratic relationship with either gods or demons, aliens or nature spirits? Are we hardwired for religious beliefs?
The shamanic personality, which is characterized by an early mental and physical healing crisis, is typically considered to have “a foot in both worlds,” the ordinary and the Great Unknown. It is this quality that makes them able to “journey” to other worlds, the underworld, or the heights. Euphoria and ecstasies come coupled with anxiety and incapacitating terror.
The psychic quality opens them to dreamlike voices and visions, premonitions, ancestral and spectral images and communications, as well as an ability to pass into and return from the realm of the dead. Feelings of oneness with all life can nurture personalities that are charismatic and create instant and powerful rapport, even spontaneous trance states and healing in others. Shamans, nature mystics or medicine people were leaders within their tribal societies.
All these qualities are correlated with the sub-clinical and TLE syndrome. Can this possibly have given rise to the ancient notion that the “falling sickness” was a “divine” disorder, dictated by the gods? Some great leaders, such as Julius Caesar, were perceived as immortals; despite the infirmity; it did not diminish and may have increased their personal power. Rather than bipolar, was Joan of Arc experiencing non-epileptic seizures or left-lobe epilepsy?
Does their seeming fearlessness arise from the intimate knowledge of the eternal “otherside.” Memory works by tapping neural networks necessary to find the information. Temporal episodes, overlapping projections of networks, can simultaneously “download” unrelated memories creating seemingly new meaningful feeling-colored experiences. They correlate with “fugue states”, flashbacks, beatific states, oceanic consciousness, and cosmic insights.
Ramachandran attributes increased emotional intensity to the kindling or potentiating of the pathway between the temporal lobe and amygdala, heightening the significance of stimuli. What is deemed meaningful becomes extraordinarily meaningful. Images of religious images or words can even be preferred over those of a sexual nature.
Some parts of the brain can block input into others. When certain portions of the brain are inhibited, such as the cingulate gyrus and orientation center, out of body experiences create a sense of floating or transport. When the parietal lobe is blocked of sensory input sense of self and world merges. The hippocampus no longer provides a “reality check.” Loss of sense of time leads to atemporal reveries and ecstasies. When cascades spread across the brain, they can entrain the auditory, visual, olfactory, or taste centers.
Overdriving the frontal cortex with induced pain, concentration or steady, regular stimulation to the CNS enhances the effect leading to disinhibition. Personal crisis, oxygen deprivation, low blood sugar, repressed serotonin levels, or fatigue amplify the process. In neurological terms, sensitization is a term meaning a stimulus that did not have an effect on the ANS now does. The effects, either anomalous or from meditation, can be spontaneous or cumulative.
This, of course, also relates directly to stress-induced syndromes. Neuroelectrical activity cranked up beyond a certain threshold creates travelling and rotating waves that form complex interference patterns (Mandell). Physical and psychological stress can cause changes in the amount of hormones secreted, affecting general health and reproductive interest and ability. Conversely hormones affect the brain.
TICKLING THE GOD MODULE
We are wired to experience God. Different researchers have slightly different names for the religious syndrome. Ramachandran calls it “the God module.” Persinger calls it the “God experience”. Both researchers indicate waves of temporal lobe excitation with hemispheric coherence underlie spiritual experience and religious belief. “The Kingdom of heaven is within.”
It is reported Dostoevsky said his seizures gave him “feelings of magnificence, abundance, eternity.” Poe and Lewis Carrol brought their novel distorted perceptions into their writing to the delight of millions. Van Gogh was prolific, though tormented, unconnective, and codependent. Writers from Tennyson to Philip K. Dick have turned their infirmity to their advantage.
When they could easily moderate them with anticonvulsants, many individuals still choose to endure their symptoms rather than relinquish glimpses of the psychic fireworks it brings. Still, neuroscientists are the first to admit that God is not reduceable to a neuroelectrical flux. But stress, particularly loss of a loved one, definitely facilitates the God experience. Elevated stress hormones can trigger the temporal lobe, amygdala, and hippocampus.
Persinger has tickled the temporal lobes of enough individuals to define the parameters of electromagnetic shifts on brain function. The recent medical use of Transcranial Magnetic Stimulation (TMS) to relieve a variety of psychological symptoms such as depression indicates that the mind may be an electromagnetic field.
Not all those with intense spiritual experiences have temporal lobe epilepsy. Meditators often sit for years before experiencing the slightest tingles or visions of light. But often once manifestations begin, they increase in frequency and tend to stabilize. They can come as sounds, smells, intense feeling, visonary landscapes or forms of living entities, or amorphous lights. These inner experiences feel as real or seem more real than external perception.
The study of how the brain creates god experiences is the province of the embryonic field of neurotheology. As the marriage of brain science with theology, it systematically describes the relationship between humans, God and the universe in neurological terms (Miller, 2003).
But just because we can say the brain declares, “Let there be God,” doesn’t mean a higher power does not exist. When God said, “Let there be Light,” perhaps it also meant the electrical impulses that vivify, provide meaning and enlighten our mundane existence. Visions cannot be judged solely on the neurological basis but must be judged for their own merit and validity. Not all visions are pathological, nor all visionaries or spiritual adepts epileptics.
Subjective experiences are the basis of mysticism and the religious impulse. The brain is hard-wired for mystical experiences, perhaps as an adaptation to soothe the stress incured in daily life. Peak experiences, raptures, epiphanies, even illumination are potentially available to everyone. Spontaneous transient electrical choas in the temporal lobes is perfectly normal, making the God experience an artifact of healthy function.
We can learn to make space, time and personality dissolve. Fear dissolves too as we kiss the feet of eternity. All we have to do is withdraw our attention from the senses and interrupt certain brain circuits. These experiences can also be induced neuromagnetically with new technologies, and non-invasively with “brainwave drivers” such as the frequency-following response or binaural beat technology (Monroe).
The god experience is a process in which one learns to embody spiritual being, infusing life with meaning. The soul soars, freed from the prison of ego, mind and body. It brings in its wake oceanic expansion, suspension of time, space and ego, sudden insight, childlike wonder, exaltation, gnosis, fusion.
Appendix & References Appendix A: The TLE Syndrome
TLE is often undiagnosed as subjects often forget a simple but crucial injury to the head, even in childhood, such as falling down stairs, car wrecks, swimming injuries, or a host of other everyday bumps and jolts. The soft temporal lobes are vulnerable to injury any time they bump against the hard skull.
Dr. Daniel Amen says temporal lobe functions include auditory processes, ventral visual stream, auditory input, visual object recognition and classification, long term storage of sensory input. It links with the amygdala which adds the emotional tone to sensory input and memories. The hippocampus helps us navigate and determine where we are in space.
Primary functions of the dominant side (usually the left) include perception of words and processing of language related sounds, sequential analysis, increased blood flow during speech perception, processing details, intermediate and long term memory, auditory learning and retrieval of words, visual and auditory processing, and complex memories.
So instabilities or damage to the left lobe create problems such as emotional instability, decreased verbal memory, difficulty categorizing words or pictures, failing to understand words in context, internally and externally driven aggression, dark or violent thoughts, sensitivity to slights and mild paranoia, auditory processing problems, and reading difficulties.
Non-dominant side (usually the right) temporal functions include perception of melodies, pitch and rhythm, social cues, reading facial expressions, and vocal intonation, visual learning, and increased blood flow during tonal memory. Problems include recall of shapes, faces, and tunes; inept social skills, trouble reading social cues and context; decreased attention to visual input; trouble processing music and visual imagery.
Problems in either or both lobes create troubles with memories, fears, confusion, anxiety, abnormal sensory perceptions, visual and auditory hallucinations, spaciness or amnesia, déjà vu and jamais vu, unusual abdominal pain or headaches, religious or moral preoccupation, excessive writing, overemphasis on trivia, and of course seizures.
Dr. Amen sums up the symptomology with ten defining points: 1). Disturbance of auditory sensation and perception; 2). Disturbance of selective attention of auditory and visual input; 3). Disorders of visual perception; 4). Impaired organization and categorization of verbal material; 5). Disturbance of language comprehension; 6). Decreased long term memory; 7). Altered personality and affective development; 8). Altered sexual behavior; 9). Inability to perceive or remember events; 10). Damage to the inferior aspect of the temporal lobe – decreased memory in proportion to tissue damaged.
APPENDIX B
Personal Philosophy Inventory (Makarec and Persinger, 1990)
(Sample items indicating complex partial epileptic temporal lobe signs.)
While sitting quietly, I have had uplifting sensations as if I were driving over a rolling road.
I often feel as if things are not real.
At least once, before falling down, I had an intense smell from childhood, apparently for no reason.
Once, in a crowded place, I suddenly could not recognize where I was.
I have had a vision.
People tell me I "blank out" sometimes when we're talking.
When relaxed or before falling asleep I sometimes feel pleasant vibrations moving through my body.
Sometimes in the very early morning hours I have meaningful experiences.
I have heard an inner voice call my name.
I use hunches more than simple learning to solve new problems.
Sometimes an event occurs that has special significance for me only.
I have had experiences where I felt as if I were somewhere else.
There have been brief times when I felt very close to a Universal Consciousness.
I have had dreams of floating or flying through the air.
At least once in my life I have felt the presence of another being.
(Sample items indicating Psi experiences or exotic beliefs)
I have been taken aboard a space ship.
I would like to time travel.
When I have a tough decision a sign will be given and I will know what to do.
If God told me to kill, I would do it in His name.
I think there is a good possibility that I have lived a previous life.
Telepathy is a real phenomenon.
An inner voice has told me where to find something and it was there.
Alien intelligence is probably responsible for UFOs.
I have felt as if I have left my body.
*****
APPENDIX C
Subjective Experiences Questionnaire (Ruttan, Persinger and Koren, 1990) {exit survey}
( Sample items indicating targeted experiences test for vestibular, depersonalization, and imaginings.)
I felt dizzy or odd.
I felt the presence of someone or something near me.
There were tingling sensations.
I saw vivid images.
There were pleasant vibrations moving through my body.
I heard an inner voice call my name or speak to me.
I experienced anger.
I experienced sadness.
The experience did not come from my own mind.
I heard a ticking sound.
There were odd smells.
I experienced terror or fear.
There were odd tastes in my mouth.
I felt as if I were somewhere else.
I experienced thoughts from childhood.
The same idea kept occurring.
I felt as if I were spinning around.
There were images from dreams I've had.
The red light became brighter or darker.
REFERENCES
Amen, Daniel C. (19 ). Change Your Brain, Change Your Life.
Amen, Daniel C. (19 ). Healing Anxiety and Depression.
Amen, Daniel C.(19 ). Healing the Hardware of the Soul:How Making the Brain-Soul Connection Can Optimize Your Life, Love and Spiritual Growth.
Bear, D. M. and Fedio, P. (1977). Quantitative Analysis of Interictal Behavior in Temporal Lobe Epilsepsy,” Archives of Neurology, 34, 1977, pp.454-467.
Begley, Sharon (2001). “Religion and the Brain”. Newsweek, April, 2001.
Blackmore, Susan (1993). Dying to Live: Near-Death Experiences. Buffalo, NY: Prometheus.
Cardena, Etzel, Lynn, Steven Jay, and Krippner, Stanley (eds.) (2001). The Varieties of Anomalous Experience. Washington D.C.: American Psychological Assn.
Cirignotta, F., Todesco, C. V., & Lugaresi, E. (1980). Temporal lobe epilepsy with ecstatic seizures (so-called Dostoevskian Epilepsy). Epilepsia, 21, 705-710.
Csikszentmihalyi, Mihaly (1990). Flow: The Psychology of Optimal Experience. New York: Harper & Row.
Gloor, P. (1982-1986). “Role of the Human Limbic System in Perception, Memory, and Affect: Lessons from Temporal Lobe Epilepsy,” Annals of Neurology, 12, 1982, pp, 129-144. Also in The Limbic System, Doane and Livingston (eds.). New York: Raven (1986).
Goleman, Daniel (1995). Emotional Intelligence. New York: Bantam.
Hobson, Alan (1998). Consciousness. Scientific American Press.Hooper, Judith and Tersi, Dick (1986). The Three-Pound Universe. New York: Tarcher/G. P. Putnam’s Sons.
Horgan, John (2003). Rational Mysticism. New York: Houghton Mifflin Company.
Huot, B., Makarec, K. & Persinger, M.A. (1989). Temporal Lobe Signs and Jungian Dimensions of Personality. Perceptual and Motor Skills, 69, 841-842.
LaPlante, Eve (1994). Seized.
Makarec, K., & Persinger, M. A. (1985). Temporal lobe signs: Electroencephalographic validity and enhanced scores in special populations. Perceptual and Motor Skills, 60, 831-842.
Makarec, K., & Persinger, M. A. (1990). Electroencephalographic validation of a temporal lobe signs inventory in a normal population. Journal of Research in Personality, 24, 323-337.
Mandell, Arnold (1980). “Toward a Psychobiology of Transcendence: God in the Brain” on Davidson & Davidson (eds.), The Psychobiology of Consciousness. New York: Plenum Press.
Marshall, E. J., Syed, G. M. S., Fenwick, P. B. C., & Lishman, W. A. (1993). A pilot study of schizophrenia-like psychosis in epilepsy using single photon emission computerized tomography. British Journal of Psychiatry, 163, 32-36.
Maturana, U. & Varela, F. (1987). The Tree of Knowledge: the Biological Roots of Human Understanding. Shambala: Boston.
McKinney, Laurence O.(1994). Neurotheology: Virtual Religion in the 21st Century. Cambridge, Mass.: American Institute for Mindfulness.
Munro, C., & Persinger, M. A. (1992). Relative right temporal lobe theta activity correlates with Vignanos Hemispheric Quotient and the sensed presence. Perceptual and Motor Skills, 75, 899-903.
Murphy, Todd (2013), Sacred Pathways: The Brain's Role in Religious and Mystical Experiences.
Niedermeyer, E. (1982). Epileptic seizure disorders. In Niedermeyer & F. L. da Silva (Eds.) Electroencephalography: Basic Principles, Clinical Applications and Related Fields, Baltimore-Munich: Urban & Swartzenberg. Pp. 339-428.
Miller, Iona (2001). “Neurotheology 101: Our Innate Capacity for Spiritual or Mystical Experience”. Asklepia Foundation.
Miller, Iona (2003). “How the Brain Creates God: the Emerging Science of Neurotheology,” Chaosophy 2003. Grants Pass, Oregon: Asklepia Press.
Moody, R.A. (1975). Life After Life. Covington, Ga.: Mockingbird Books.
Monroe, Robert
Okamura, A. O., Fukai, M., Yamadori, A., Hidari, M., Asaba, H., & Sakai, T. (1993). A clinical study of hypergraphia in epilepsy. Journal of Neurology, Neurosurgery, and Psychiatry, 56, 556-559.
Perez, M. M., Trimble, M. R., Murray, N. M. F., & Reider, I. (1985). Epileptic psychosis: An evaluation of PSE profiles. British Journal of Psychiatry, 146, 155-163
Persinger, M. A. (1975). “ELF Waves and ESP”; New Horizons, I(5), January 1975, pp.232-235.
Persinger, M. A. , (1983). Religious and mystical experiences as artifacts of temporal lobe function. Perceptual and Motor Skills, 57, 1255-1262.
Persinger, M. A. , (1984). Striking EEG profiles from single episodes of glossolalia and transcendental meditation. Perceptual and Motor Skills, 58, 963-975.
Persinger, M. A. , (1984). People who report religious experiences may also display enhanced temporal lobe signs. Perceptual and Motor Skills. 58, 963-975.
Persinger, M. A. , (1985). Geophysical variables and human behavior: XXX. Intense paranormal experiences occur during days of quiet, global geomagnetic activity. Perceptual and Motor Skills, 61, 320-322.
Persinger, M. A., & Valliant, P. M. (1985). Temporal lobe signs and reports of subjective paranormal experiences in a normal population: A replication. Perceptual and Motor Skills, 60, 903-909.
Persinger, Michael A. (1987). Neuropsychological Bases of God Beliefs. New York: Praeger Publishers.
Persinger, M. A. and Makarec, K. (1987). “Temporal Lobe Epilsepsy Signs and Correlative Behaviors Displayed by Normal Populations,” Journal of General Psychology, 114, 1987, pp. 179-185.
Persinger, M. A. , (1988). Temporal lobe signs and personality characteristics. Perceptual and Motor Skills, 66, 49-50.
Persinger, Michael (1989). “Psi Phenomena and Temporal Lobe Activity: The Geomagnetic Factor,” in L.A. Henkel and R. E. Berger (eds.), Research in Parapsychology 1988; Metuchen, NJ: Scarecrow Press, 1989.
Persinger, M. A., & Fisher, S. D. (1990). Elevated, specific temporal lobe signs in a population engaged in psychic studies. Perceptual and Motor Skills, 71, 817-818.
Persinger, M. A., Koren, S. A., Makarec, K., Richards, P., & Youlton, S. (1991). Differential effects of wave form and the subjects possible temporal lobe signs upon experiences during cerebral exposure to weak intensity magnetic fields. Journal of Bioelectricity, 10(1&2), 141-184.
Persinger, M. A. , (1991). Subjective pseudocyesis (false pregnancy) and elevated temporal lobe signs: An implication. Perceptual and Motor Skills, 72, 499-503.
Persinger, M. A. , (1993). Transcendental meditation and general meditation are associated with enhanced complex partial epileptic-like signs: Evidence for cognitive kindling? Perceptual and Motor Skills, 76, 80-82.
Pribram, Karl H. (1971). Languages of the Brain: Experimental Paradoxes and Principles in Neuropsychology. Monterey, Calif.: Brooks/Cole Publishing Co.
Ramachandran, Vilayanur (1998). Phantoms in the Brain.
Richards, P. M., Koren, S. A., & Persinger, M. A. (1992). Experimental stimulation by burst-firing weak magnetic fields over the right temporal lobe may facilitate apprehension in women. Perceptual and Motor Skills, 75, 667-670.
Ring, Kenneth (1984). “The Nature of Personal Identity in the Near-Death Experience”. Anabiosis 4(1) (Spring 1984).
Ruttan, L. A., Persinger, M. A. & Koren, S. A. (1990). Enhancement of temporal lobe-related experiences during brief exposures to milligauss intensity extremely low frequency magnetic fields. Journal of Bioelectricity, 9(1), 33-54.
Ryvlin, P., Philipon, B., Cinotti, L., Froment, J. C., LeBars, D., & Mauguiere, F. (1992). Functional neuroimaging strategy in temporal lobe epilepsy: A comparative study of 18FDG-PET and 99MtC-HMPAO- SPECT. Annals of Neurology, 31(6), 650-656.
Saavedra-Aguilar, J.C. & Gomez-Jeria, J.S. (1989). “A Neurobiological Model for Near-Death Experiences.” Journal of Near-Death Studies, 7, 205-222.
Sabom, M (1982). Recollections of Death: A Medical Investigation. New York: Harper & Row.
Sabom, M. (1998). Light and Death: One Doctor’s Fascinating Account of Near-Death Experiences. Grand Rapids, MI: Zondervan.
Salzman, Mark. Lying Awake.
Strassman, Rick (1997). “Endogenous ketmine-like compounds and the NDE…” Journal of Near-Death Studies, 16, 27-41.
Strassman, Rick (2001). DMT: The Spirit Molecule. Rochester, Vermont: Park St. Press.
Varela, F., Thompson, E. & Rosch, E. (1991). The Embodied Mind. MIT Press: Boston.
Waller, N. G., Kojetin, B. A., Bouchard Jr., T. J., Lykken, D. T., & Tellegen, A. (1990). Genetic and environmental influences on religious interests, attitudes and values. Psychological Science, 1(2), 138-142.
File Created: 9-14-03
Extended References:
Allen, J., & Lester, D. (1994). Belief in paranormal phenomena and an external locus of control. Perceptual and Motor Skills, 79, 226.
Arango, M. A. , & Persinger , M. A. (1988). Geophysical variables and behavior: LII. Decreased geomagnetic activity and spontaneous telepathic experiences from the Sidgwick collection. Perceptual and Motor Skills, 67, 907-910.
Ardilla, A. (1989). Partial cognitive seizures . Neuropsychiatry, Neuropsychology, and Behavioral Neurology, 2(3), 175-182.
Berger, R. E., & Persinger , M. A. (1991). Geophysical variables and behavior: LXVII. Quieter annual geomagnetic activity and larger effect size for experimental psi (ESP) studies over six decades. Perceptual and Motor Skills, 73, 1219-1223.
Brewerton, T. D. (1994). Hypereligiosity in psychotic disorders. The Journal of Nervous and Mental Disease, 182(5), 302-304.
Gillis, C., & Persinger, M. A. (1993). Shifts in the Plutchik Emotion Profile indices following three weekly treatments with pulsed Vs continuous cerebral magnetic fields. Perceptual and Motor Skills, 76, 168-170.
Hopping, M. (1984). Psychic seizures: A diagnostic challenge. Bulletin of the Menninger Clinic, 48(5), 401-417.
Kalat, J. W. (1995). Biological Psychology (5th. Ed.). Pacific Grove: Brookes/Cole.
Kumar, V. K., Pekala, R. J., & Cummings, J. (1993). Sensation seeking, drug use and paranormal beliefs and experiences. Personality and Individual Differences, 14(5), 685-691.
Ogunyemi, A. O., & Breen, H. (1993). Seizures induced by music. Behavioral Neurology, 6, 215-218.
Pederson, D. M. (1994). Identification of levels of self-identity. Perceptual and Motor Skills, 78, 1155-1167.
Persinger, M. A. , (1983). Geophysical variables and human behavior: VII. Specific prediction of UFO reports within the New Madrid states by solar-geomagnetic and seismic measures. Perceptual and Motor Skills, 56, 243-249.
Persinger, M. A. , (1992). Neuropsychological profiles of adults who report sudden remembering of early childhood experiences: Implications for claims of sex abuse and alien visitation/abduction experiences. Perceptual and Motor Skills, 75, 254-266.
Persinger, M. A. , (1993). Average diurnal changes in melatonin levels are associated with hourly incidence of bereavement apparitions: Support for the hypothesis of temporal (limbic) lobe microseizuring. Perceptual and Motor Skills, 76, 444-446.
Persinger, M. A. , (1993). Geophysical variables and human behavior: LXXI. Differential contribution of geomagnetic activity to paranormal experiences concerning death and crises: An alternative to the ESP hypothesis. Perceptual and Motor Skills, 76, 555-562.
Persinger, M. A., & Derr, J. S. (1984). Geophysical variables and human behavior: XIX. Strong temporal relationships between inclusive seismic measures and UFO reports within Washington state. Perceptual and Motor Skills, 59, 551-566.
Persinger, M. A., & Levesque, B. F. (1983). Geophysical variables and human behavior: XII. The weather matrix accommodates large portions of variance of measured daily mood. Perceptual and Motor Skills, 57, 868-870.
Rank, O. (1971). The Double: A Psychoanalytic Study, trans. by Harry Tucker Jr., Chapel Hill: University of North Carolina.
Richards, P. M., Persinger, M. A. & Koren, S. A. (1993). Modification of activation and evaluation properties of narratives by weak complex magnetic field patterns that simulate limbic burst firing. International Journal of Neuroscience, 71, 71-85.
Schaut, G. B., & Persinger, M. A. (1985). Geophysical variables and human behavior: XXXI. Global geomagnetic activity during spontaneous paranormal experiences: A replication. Perceptual and Motor Skills, 61, 412-414.
Tobacyk, J. J., & Wilkinson, L. V. (1991). Paranormal beliefs and preferences for games of chance. Psychological Reports, 68, 1088-1090.
Waller, N. G., Kojetin, B. A., Bouchard Jr., T. J., Lykken, D. T., & Tellegen, A. (1990). Genetic and environmental influences on religious interests, attitudes and values. Psychological Science, 1(2), 138-142.
The current hypothesis is that Positron Emission Tomography can demonstrate which specific limbic structures are involved in the expression of these altered states on an approximately linear relationship between the continuum of emotionality and the continuum of involvement of cerebral structures ranging from cortical temporal lobe to hippocampal/amygdaloid structures to core basal limbic structures; in effect, the deeper the activation, the deeper the emotion. Retention of the null hypothesis would require either a) subjects who represent a normal population demonstrate no affective experiences on the SEQ as a result of the stimulus, or b) affective experiences are reported but limbic regions are not shown to be involved.
NEAR DEATH EXPERIENCE RESEARCH
http://www.stnews.org/News-787.htm
Having a near death experience can change a person’s entire life, including one’s brain, researchers have discovered.
Researcher Willoughby Britton, a doctoral student at the University of Arizona, studied the brain waves of people who have had positive, transformative near death experiences and found their brain patterns distinctive when compared with people who didn’t have a brush with death.
“It’s interesting to see why some people are transformed and why some people aren’t and whether studying people with positive near death experiences can help the people who have negative experiences,” Britton said. “It’s a profound personality overhaul.”
Britton compared the brainwaves of sleeping subjects and found a distinct spike in activity in the temporal lobe of people with near death experiences.
The brain’s temporal lobe has often been implicated in reports of near death experiences that closely mirror what epileptics feel during a seizure: feelings of peace and tranquility, encountering a bright light and increased sensitivity to smells and sounds.
The temporal lobe, Britton said, is considered “the God module, the part of the brain that connects with the transcendent.” Surprisingly, however, all of the activity that Britton recorded was from the left half of the brain not the right half, which is more often associated with visual and spatial creativity.
“One hundred percent of the activity came from the left side, which, in itself, is very unusual,” said Britton. “There’s no reason for someone to have an accident and just have one side of their brain affected.”
All those in Britton’s study who came close to dying scored higher on an evaluation of their ability to cope with stressful situations than their counterparts.
http://query.nytimes.com/gst/fullpage.html?sec=health&res=9D06E4DE1E38F930A25757C0A9629C8B63
The scientists assumed that the near-death group would show patterns of brain activity similar to those seen in temporal lobe epileptics, who often describe undergoing spiritual out-of-body events during seizures. The abnormal activity, however, did not spring up in the right temporal lobe, as is sometimes the case with epilepsy. Instead, the activity appeared almost exclusively in the left temporal lobe.
Unexpectedly, the researchers also found that the participants, like many people who suffer depression, had abnormal sleep patterns. But unlike people with depression, who move unusually quickly into the rapid eye movement or REM phase of sleep, the subjects who reported near-death experiences took an unusually long time to move into REM.
PDF: Near-Death Experiences and the Temporal Lobes by Willoughby Britton
http://matrix.aklab.psych.ubc.ca/uploads/Amelia_Neardeath_PS.pdf#search=%22temporal%20lobes%20willoughby%20britton%22
Perceptual and Motor Skills, 1983, 57, 1255-1262. © Perceptual and Motor Skills 1983
RELIGIOUS AND MYSTICAL EXPERIENCES AS ARTIFACTS OF
TEMPORAL LOBE FUNCTION: A GENERAL HYPOTHESIS
Micheal A. Persinger
Laurentian University
Summary: Mystical and religious experiences are hypothesized to be evoked by transient, electrical microseizures within deep structures of the temporal lobe. Although experiential details are affected by context and reinforcement history, basic themes reflect the inclusion of different amygdaloid-hippocampal structures and adjacent cortices. Whereas the unusual electrical coherence allows access to infantile memories of parents, a source of god expectations, specific stimulation evokes out-of-body experiences, space-time distortions, intense meaningfulness, and dreamy scenes. The species-specific similarities in temporal lobe properties enhance the homogeneity of cross- cultural experiences. They exist along a continuum that ranges from “early morning highs” to recurrent bouts of conversion and dominating religiosity. Predisposing factors include any biochemical or genetic factors that produce temporal lobe lability. A variety of precipitating stimuli provoke these experiences, but personal (life) crises and death bed conditions are optimal. These temporal lobe microseizures can be learned as responses to existential trauma because stimulation is of powerful intrinsic reward regions and reduction of death anxiety occurs. The implications of these transients as potent modifiers of human behavior are considered.
The neuropsychological basis of religious experiences and God beliefs has avoided by behavioral scientists. Yet these experiences, in conjunction the confrontation and attenuation of death anxiety, constitute a major class of human behaviors whose frequency is rivaled only by sex and aggression. This paper briefly describes a general hypothesis that religious and mystical experiences are normal consequences of spontaneous biogenic stimulation of temporal lobe structures. The numbers, composition, and intensity of these experiences reflect a continuum of temporal lobe stability. Each human being may be located somewhere along this dimension.
The temporal lobe of the human brain is an optimal locus for the creation of religious experiences. Cortical and deep structures (primarily the amygdaloid and hippocampal complexes) are associated with the sense of “self” in relationship to time and space, the memory-dependent conception of their limits primary affective components of anticipation, especially of nociceptive events. Given copious inputs from languaging centers (Gloor, 1972), all of these experiences are influenced by suggestion and by the rich imagery-evoking sequences of metaphorical language. It is not surprising that anticipation of self-dissolution, death anxiety, would emerge within this context.
Deep telencephalic structures have acquired particular importance in human development. Experiences of self and the propensity for self-preservation have been elaborated upon the general amygdaloid role of hypothalamic modulation. The amygdala contains representations of motivational states and their affective (pleasure or reward versus pain or punishment) dimensions. Whereas crude (and wide spread) stimulation evokes fear (Weingarten, Cherlow, & Holmgren, 1977) and general anxiety (anticipation of negative stimuli), more subtle stimulation evokes intense meaningfulness and peak experiences; the latter are often in conjunction with altered body perceptions, such as out-of-body experiences (Jasper & Rasmussen, 1958) or convictions of cosmic communion.
Intricate and highly organized connections between deep structures and the overlying associative cortices allow complex memories and language to control the evocation of amygdaloid experiences. Consequently, they can be infused with the details of context and determined by the expectancy of the person. Plentiful opiate receptor sites in this portion of the amygdala and along the temporal pole (Pay, 1982) allow positive experiences to be influenced by a chemical dimension that ranges from synthetic substances (morphine derivatives) to the enkephalin physiology of life crises.
Considering the direct connections to the dorsomedial portions of the thalamus and orbital frontal lobes, time distortions (e.g., viewing eternity in a split second) would not be unexpected. Sudden amygdaloid stimulation and alteration of the sense of self in space-time could momentarily alter hippocampal function and change memory reference. The alteration may range from institution of memories that appear to be “old and real” to the conviction that something meaningful and intensely personal has happened (although the details are vague). A significant portion of them would be characterized by a long latency between the time of the experience and its report.
Three important physiological properties target the temporal lobe as the source of mystical/religious experiences. Post-stimulation electrical instability, an intrinsic feature of deep structures, allows the creation of transient neuronal firing patterns that do not necessarily represent concurrent sensory input. Instead, they could incorporate combinations of memory and fantasy, but still within the context of the moment. This region is well known for its capacity to generate learned seizures (kindling); antithetically, conditioned inhibition of seizure patterns, is also predictable and has been observed (Efron, 1957).
Second, these areas are prone to vascular anomalies such as transient vasospasms. They are now considered a primary cause of hallucinatory experiences (Altura & Altura, 1981). The recent evolutionary changes in the position of Ammon’s horn, including the formation of an extra gyrus to accommodate this development, has fostered vasospasmogenic potential due to the odd cytoarchitecture. This is enhanced by the conspicuous coronal asymmetry of the Sylvian fissures (LeMay, 1982) which contribute to unusual electrical discrepancies between the two hemispheres.
The plasticity of temporal lobe neuronal and glial populations are exceptional. Cellular membranes in this region are prone to both interneuronal and neuronal-glial fusion, an important predisposing factor to psychomotor epilepsy (Schwartzkroin, 1983); within less extreme conditions, it aids unusual mixtures of cell ensembles. They can be affected by vitamin B deficiencies, hormonal fluctuations, hypoglycemia, hypoxia, and tumorogenesis, to which these structures are particularly sensitive (Breggin, 1979). Although postnatal neurogenesis has not been clearly demonstrated in man, this area displays environmental-dependent alterations in dendritic arborbization that are evident even by light microscopy (Buell & Coleman, 1979).
According to the hypothesis, the actual mystical or religious experience is evoked by a transient (a few seconds), very focal, electrical display within the temporal lobe. Such temporal lobe transients (TLTs) would be analogous to electrical microseizures without any obvious motor components; some facial expressions, such as ecstasy and occasional lacrimation would be noticeable. Lip smacking, facial distortions, automatisms, and vagal glossopharyngeal-mediated vocalization (speaking in tongues), followed by amnesia, would occur in more extreme conditions. Although most TLTs should be subcortical in origin, some would be represented within electroencephalic (EEG) profiles. They would be characterized by local, perhaps even lead- specific, transient, seizure-like signatures surrounded by normal activity.
